Pancreaticoduodenectomy
A pancreaticoduodenectomy, also known as a Whipple procedure, is a major surgical operation most often performed to remove cancerous tumours off the head of the pancreas.[2] It is also used for the treatment of pancreatic or duodenal trauma, or chronic pancreatitis.[2] Due to the shared blood supply of organs in the proximal gastrointestinal system, surgical removal of the head of the pancreas also necessitates removal of the duodenum, proximal jejunum, gallbladder, and, occasionally, part of the stomach.[2]
| Pancreaticoduodenectomy | |
|---|---|
 The pancreas, stomach, and bowel are joined back together after a pancreaticoduodenectomy | |
| Other names | Pancreatoduodenectomy,[1] Whipple procedure, Kausch-Whipple procedure |
| ICD-9-CM | 52.7 |
| MeSH | D016577 |
Anatomy involved in the procedure
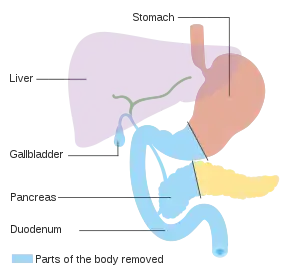

The most common technique of a pancreaticoduodenectomy consists of the en bloc removal of the distal segment (antrum) of the stomach, the first and second portions of the duodenum, the head of the pancreas, the common bile duct, and the gallbladder. Lymph nodes in the area are often removed during the operation as well (lymphadenectomy). However, not all lymph nodes are removed in the most common type of pancreaticoduodenectomy because studies showed that patients did not benefit from the more extensive surgery.[3]
At the very beginning of the procedure, after the surgeons have gained access to the abdomen, the surfaces of the peritoneum and the liver are inspected for disease that has metastasized. This is an important first step as the presence of active metastatic disease is a contraindication to performing the operation.
The vascular supply of the pancreas is from the celiac artery via the superior pancreaticoduodenal artery and the superior mesenteric artery from the inferior pancreaticoduodenal artery. There are additional smaller branches given off by the right gastric artery which is also derived from the celiac artery. The reason for the removal of the duodenum along with the head of the pancreas is that they share the same arterial blood supply (the superior pancreaticoduodenal artery and inferior pancreaticoduodenal artery). These arteries run through the head of the pancreas, so that both organs must be removed if the single blood supply is severed. If only the head of the pancreas were removed it would compromise blood flow to the duodenum, resulting in tissue necrosis.
While blood supply to the liver is left intact, the common bile duct is removed. This means that while the liver remains with a good blood supply the surgeon must make a new connection to drain bile produced in the liver. This is done at the end of the surgery. The surgeon will make a new attachment between the pancreatic duct and the jejunum or stomach. During the surgery a cholecystectomy is performed to remove the gallbladder. This portion is not done en bloc, as the gallbladder is removed separately.
Relevant nearby anatomy not removed during the procedure include the major vascular structures in the area: the portal vein, the superior mesenteric vein, and the superior mesenteric artery, the inferior vena cava. These structures are important to consider in this operation especially if done for resection of a tumor located in the head of the pancreas. If the tumor encases (wraps around 50% or more of the vessel) the celiac artery, superior mesenteric artery, or inferior vena cava it is considered unresectable due to the lack of patient benefit from the operation while having very high risk.[4][5] Occasionally a portion of the superior mesenteric vein or portal vein is attached or inseparable from the tumor. In this setting vascular surgeons resect the involved portion of the vessel, and the vessel is repaired either via end-to-end anastomosis, repair of the side wall of the vein, or a vein graft.
Medical indications
Pancreaticoduodenectomy is most often performed as curative treatment for periampullary cancer, which include cancer of the bile duct, duodenum or head of the pancreas.[6] The shared blood supply of the pancreas, duodenum and common bile duct, necessitates en bloc resection of these multiple structures. Other indications for pancreaticoduodenectomy include chronic pancreatitis, benign tumors of the pancreas, cancer metastatic to the pancreas, multiple endocrine neoplasia type 1[7] and gastrointestinal stromal tumors.[6]
Pancreatic cancer
Pancreaticoduodenectomy is the only potentially curative intervention for malignant tumors of the pancreas.[8] However, the majority of patients with pancreatic cancer present with metastatic or locally advanced unresectable disease;[9] thus only 15-20% of patients are candidates for the Whipple procedure. Surgery may follow neoadjuvant chemotherapy, which aims to shrink the tumor and increasing the likelihood of complete resection.[10] Post-operative death and complications associated with pancreaticoduodenectomy have become less common over the past 20 years, with rates of post-operative mortality falling from 10-30% in the 1980s, to less than 5% in the 2000s.[11]
Cholangiocarcinoma
Cholangiocarcinoma, or cancer of the bile duct, is an indication for the Whipple procedure when the cancer is present in the distal biliary system, usually the common bile duct that drains into the duodenum. Depending on the location and extension of the cholangiocarcinoma, curative surgical resection may require hepatectomy, or removal of part of the liver, with or without pancreaticoduodenectomy.[12]
Chronic pancreatitis
Treatment of chronic pancreatitis typically includes pain control and management of exocrine insufficiency. Intractable abdominal pain is the main surgical indication for surgical management of chronic pancreatitis.[13] Removal of the head of the pancreas can relieve pancreatic duct obstruction associated with chronic pancreatitis.[14]
Trauma
Damage to the pancreas and duodenum from blunt abdominal trauma is uncommon. In rare cases when this pattern of trauma has been reported, it has been seen as a result of a lap belt in motor vehicle accidents.[15] Pancreaticoduodenectomy has been performed when abdominal trauma has resulted in bleeding around the pancreas and duodenum, damage to the common bile duct, pancreatic leakage, or transection of the duodenum.[16] Due to the rarity of this procedure in the setting of trauma, there is not robust evidence regarding post-operative outcomes.
Contraindications
Absolute contraindications for the procedure are metastatic disease in the abdominal cavity or nearby organs. These are found most often on the peritoneum, in the liver, and in the omentum. In order to determine if there are metastases, surgeons will inspect the abdomen at the beginning of the procedure after gaining access. Alternatively, they may perform a separate procedure called a diagnostic laparoscopy which involves insertion of a small camera through a small incision to look inside the abdomen. This may spare the patient the large abdominal incision that would occur if they were to undergo the initial part of a pancreaticoduodenectomy that was cancelled due to metastatic disease.
Further contraindications include encasement of major vessels (such as celiac artery, inferior vena cava, or superior mesenteric artery) as mentioned above.
Surgical considerations
Pylorus-sparing pancreaticoduodenectomy
Clinical trials have failed to demonstrate significant survival benefits of total pancreatectomy, mostly because patients who submit to this operation tend to develop a particularly severe form of diabetes mellitus called brittle diabetes. Sometimes the pancreaticojejunostomy may not hold properly after the completion of the operation and infection may spread inside the patient. This may lead to another operation shortly thereafter in which the remainder of the pancreas (and sometimes the spleen) is removed to prevent further spread of infection and possible morbidity. In recent years the pylorus-preserving pancreaticoduodenectomy (also known as Traverso-Longmire procedure/PPPD) has been gaining popularity, especially among European surgeons. The main advantage of this technique is that the pylorus, and thus normal gastric emptying, should in theory be preserved.[17] There is conflicting data as to whether pylorus-preserving pancreaticoduodenectomy is associated with increased likelihood of gastric emptying.[18][19] In practice, it shows similar long-term survival as a Whipple's (pancreaticoduodenectomy + hemigastrectomy), but patients benefit from improved recovery of weight after a PPPD, so this should be performed when the tumour does not involve the stomach and the lymph nodes along the gastric curvatures are not enlarged.[19]
Compared to the standard Whipple procedure, the pylorus preserving pancreaticoduodenectomy technique is associated with shorter operation time and less intraoperative blood loss, requiring less blood transfusion. Post-operative complications, hospital mortality and survival do not differ between the two methods.[20][21][22]
Morbidity and mortality
Pancreaticoduodenectomy is considered, by any standard, to be a major surgical procedure.
Many studies have shown that hospitals where a given operation is performed more frequently have better overall results (especially in the case of more complex procedures, such as pancreaticoduodenectomy). A frequently cited study published in The New England Journal of Medicine found operative mortality rates to be four times higher (16.3 v. 3.8%) at low-volume (averaging less than one pancreaticoduodenectomy per year) hospitals than at high-volume (16 or more per year) hospitals. Even at high-volume hospitals, morbidity has been found to vary by a factor of almost four depending on the number of times the surgeon has previously performed the procedure.[23] de Wilde et al. have reported statistically significant mortality reductions concurrent with centralization of the procedure in the Netherlands.[24]
One study reported actual risk to be 2.4 times greater than the risk reported in the medical literature, with additional variation by type of institution.[25]
Postoperative complications
Three of the most common post-operative complications are: delayed gastric emptying, bile leak, and pancreatic leak. Delayed gastric emptying, normally defined as an inability to tolerate a regular diet by the end of the first post-op week and the requirement for nasogastric tube placement, occurs in approximately 17% of operations.[26][27] During the surgery, a new biliary connection (normally a choledochal-jejunal anastamosis connecting the common bile duct and jejunum) is made. This new connection may leak in 1-2% of operations. As this complication is fairly common, it is normal in this procedure for the surgeon to leave a drain in place at the end. This allows for detection of a bile leak via elevated bilirubin in the fluid drained. Pancreatic leak or pancreatic fistula, defined as fluid drained after postoperative day 3 that has an amylase content greater than or equal to 3 times the upper limit of normal, occurs in 5-10% of operations,[28][29] although changes in the definition of fistula may now include a much larger proportion of patients (upwards of 40%).[30]
Recovery after surgery
Immediately after surgery, patients are monitored for return of bowel function and appropriate closed-suction drainage of the abdomen.
Return of bowel function
Ileus, which refers to functional obstruction or aperistalsis of the intestine, is a physiologic response to abdominal surgery, including the Whipple procedure.[31] While post-operative ileus is typically self-limited, prolonged post-operative ileus occurs when patients develop nausea, abdominal distention, pain or intolerance of food by mouth.[32] Various measures are taken in the immediate post-operative period to minimize prolonged post-operative ileus. A nasogastric tube is typically maintained to suction, to drain gastric and intestinal contents. Ambulation is encouraged to stimulate return of bowel function. Use of opioid medications, which interfere with intestinal motility, are limited.[33]
History
This procedure was originally described by Alessandro Codivilla, an Italian surgeon, in 1898. The first resection for a periampullary cancer was performed by the German surgeon Walther Kausch in 1909 and described by him in 1912. It is often called Whipple's procedure or the Whipple procedure, after the American surgeon Allen Whipple who devised an improved version of the surgery in 1935 while at Columbia-Presbyterian Medical Center in New York[34] and subsequently came up with multiple refinements to his technique.
Nomenclature
Fingerhut et al. argue that while the terms pancreatoduodenectomy and pancreaticoduodenectomy are often used interchangeably in the medical literature, scrutinizing their etymology yields different definitions for the two terms.[1] As a result, the authors prefer pancreatoduodenectomy over pancreaticoduodenectomy for the name of this procedure, as strictly speaking pancreaticoduodenectomy should refer to the resection of the duodenum and pancreatic duct rather than the pancreas itself.[1]
See also
References
- Fingerhut, A; Vassiliu, P; Dervenis, C; Alexakis, N; Leandros, E (2007). "What is in a word: Pancreatoduodenectomy or pancreaticoduodenectomy?". Surgery. 142 (3): 428–9. doi:10.1016/j.surg.2007.06.002. PMID 17723902.
- Reber, Howard (24 October 2016). "Surgical resection of lesions of the head of the pancreas". UpToDate. Retrieved 12 March 2017.
- Sun, J; Yang, Y; Wang, X; Yu, Z; Zhang, T; Song, J; Zhao, H; Wen, J; Du, Y; Lau, WY; Zhang, Y (October 2014). "Meta-analysis of the efficacies of extended and standard pancreatoduodenectomy for ductal adenocarcinoma of the head of the pancreas". World J Surg. 38 (10): 2708–15. doi:10.1007/s00268-014-2633-9. PMID 24912627.
- "Pancreatic Cancer Stages". Cancer.org. American Cancer Society. Retrieved 13 December 2017.
- "Pancreas Cancer Staging" (PDF). Cancer Staging. American Joint Committee on Cancer. Retrieved 13 December 2017.
- Cameron, John L.; Riall, Taylor S.; Coleman, JoAnn; Belcher, Kenneth A. (July 2006). "One thousand consecutive pancreaticoduodenectomies". Annals of Surgery. 244 (1): 10–15. doi:10.1097/01.sla.0000217673.04165.ea. ISSN 0003-4932. PMC 1570590. PMID 16794383.
- , Lillemoe K, Loehrer A. Whipple procedure for multiple endocrine neoplasia of the pancreas. J Med Ins. 2018;2018(16). doi:https://doi.org/10.24296/jomi/16.
- Clancy, Thomas E. (August 2015). "Surgery for Pancreatic Cancer". Hematology/Oncology Clinics of North America. 29 (4): 701–716. doi:10.1016/j.hoc.2015.04.001. ISSN 1558-1977. PMID 26226905.
- O Kane, Grainne M.; Knox, Jennifer J. (2017-11-16). "Locally advanced pancreatic cancer: An emerging entity". Current Problems in Cancer. 42 (1): 12–25. doi:10.1016/j.currproblcancer.2017.10.006. ISSN 1535-6345. PMID 29153290.
- Wolff, Robert A. (February 2018). "Adjuvant or Neoadjuvant Therapy in the Treatment in Pancreatic Malignancies: Where Are We?". The Surgical Clinics of North America. 98 (1): 95–111. doi:10.1016/j.suc.2017.09.009. ISSN 1558-3171. PMID 29191281.
- Garcea, Giuseppe; Dennison, Ashley R.; Pattenden, Clare J.; Neal, Christopher P.; Sutton, Christopher D.; Berry, David P. (2008-03-08). "Survival following curative resection for pancreatic ductal adenocarcinoma. A systematic review of the literature". Journal of the Pancreas. 9 (2): 99–132. ISSN 1590-8577. PMID 18326920.
- Tsuchikawa, Takahiro; Hirano, Satoshi; Okamura, Keisuke; Matsumoto, Joe; Tamoto, Eiji; Murakami, Soichi; Nakamura, Toru; Ebihara, Yuma; Kurashima, Yo (March 2015). "Advances in the surgical treatment of hilar cholangiocarcinoma". Expert Review of Gastroenterology & Hepatology. 9 (3): 369–374. doi:10.1586/17474124.2015.960393. ISSN 1747-4132. PMID 25256146.
- Zhao, Xin; Cui, Naiqiang; Wang, Ximo; Cui, Yunfeng (March 2017). "Surgical strategies in the treatment of chronic pancreatitis: An updated systematic review and meta-analysis of randomized controlled trials". Medicine. 96 (9): e6220. doi:10.1097/MD.0000000000006220. ISSN 1536-5964. PMC 5340451. PMID 28248878.
- Gurusamy, Kurinchi Selvan; Lusuku, Charnelle; Halkias, Constantine; Davidson, Brian R. (2016-02-03). "Duodenum-preserving pancreatic resection versus pancreaticoduodenectomy for chronic pancreatitis" (PDF). The Cochrane Database of Systematic Reviews. 2: CD011521. doi:10.1002/14651858.CD011521.pub2. ISSN 1469-493X. PMID 26837472.
- van der Wilden, Gwendolyn M.; Yeh, D. Dante; Hwabejire, John O.; Klein, Eric N.; Fagenholz, Peter J.; King, David R.; de Moya, Marc A.; Chang, Yuchiao; Velmahos, George C. (February 2014). "Trauma Whipple: do or don't after severe pancreaticoduodenal injuries? An analysis of the National Trauma Data Bank (NTDB)". World Journal of Surgery. 38 (2): 335–340. doi:10.1007/s00268-013-2257-5. ISSN 1432-2323. PMID 24121363.
- Gulla, Aiste; Tan, Wei Phin; Pucci, Michael J.; Dambrauskas, Zilvinas; Rosato, Ernest L.; Kaulback, Kris R.; Pundzius, Juozas; Barauskas, Giedrius; Yeo, Charles J. (January 2014). "Emergent pancreaticoduodenectomy: a dual institution experience and review of the literature". The Journal of Surgical Research. 186 (1): 1–6. doi:10.1016/j.jss.2013.07.057. ISSN 1095-8673. PMID 24011528.
- Testini, M; Regina, G; Todisco, C; Verzillo, F; Di Venere, B; Nacchiero, M (1998). "An unusual complication resulting from surgical treatment of periampullary tumours". Panminerva Medica. 40 (3): 219–22. PMID 9785921.
- Hüttner, FJ; Fitzmaurice, C; Schwarzer, G; Seiler, CM; Antes, G; Büchler, MW; Diener, MK (2016). "Pylorus-preserving pancreaticoduodenectomy (pp Whipple) versus pancreaticoduodenectomy (classic Whipple) for surgical treatment of periampullary and pancreatic carcinoma". Cochrane Database Syst Rev. 2: CD006053. doi:10.1002/14651858.CD006053.pub6. PMC 4356182. PMID 26905229.
- Michalski, Christoph W; Weitz, JüRgen; Büchler, Markus W (2007). "Surgery Insight: Surgical management of pancreatic cancer". Nature Clinical Practice Oncology. 4 (9): 526–35. doi:10.1038/ncponc0925. PMID 17728711.
- Karanicolas, PJ; Davies, E; Kunz, R; Briel, M; Koka, HP; Payne, DM; Smith, SE; Hsu, HP; Lin, PW (2007). "The pylorus: Take it or leave it? Systematic review and meta-analysis of pylorus-preserving versus standard whipple pancreaticoduodenectomy for pancreatic or periampullary cancer". Annals of Surgical Oncology. 14 (6): 1825–34. doi:10.1245/s10434-006-9330-3. PMID 17342566.
- Diener, MK; Knaebel, HP; Heukaufer, C; Antes, G; Büchler, MW; Seiler, CM (2007). "A systematic review and meta-analysis of pylorus-preserving versus classical pancreaticoduodenectomy for surgical treatment of periampullary and pancreatic carcinoma". Annals of Surgery. 245 (2): 187–200. doi:10.1097/01.sla.0000242711.74502.a9. PMC 1876989. PMID 17245171.
- Iqbal, N; Lovegrove, RE; Tilney, HS; Abraham, AT; Bhattacharya, S; Tekkis, PP; Kocher, HM (2008). "A comparison of pancreaticoduodenectomy with pylorus preserving pancreaticoduodenectomy: A meta-analysis of 2822 patients". European Journal of Surgical Oncology. 34 (11): 1237–45. doi:10.1016/j.ejso.2007.12.004. PMID 18242943.
- "The Whipple Procedure". Pri-Med Patient Education Center. Harvard Health Publications. 2009. Archived from the original on 27 July 2011.
- De Wilde, R.F.; et al. (2012). "Impact of nationwide centralization of pancreaticoduodenectomy on hospital mortality". The British Journal of Surgery. 99 (3): 404–410. doi:10.1002/bjs.8664. PMID 22237731.
- Syin, Dora; Woreta, Tinsay; Chang, David C.; Cameron, John L.; Pronovost, Peter J.; Makary, Martin A. (2007). "Publication Bias in Surgery: Implications for Informed Consent". Journal of Surgical Research. 143 (1): 88–93. doi:10.1016/j.jss.2007.03.035. PMID 17950077.
- Wente, Moritz; Bassi, Claudio; Dervenis, Christos; Fingerhut, Abe; Gouma, Dirk; Izbicki, Jakob; Neoptolemos, John; Padbury, Robert; Sarr, Michael; Traverso, L. William; Yeo, Charles; Buchler, Markus (Nov 2007). "Delayed gastric emptying (DGE) after pancreatic surgery: A suggested definition by the International Study Group of Pancreatic Surgery (ISGPS)". Surgery. 142 (5): 761–768. doi:10.1016/j.surg.2007.05.005. PMID 17981197.
- Traverso, L; Hashimoto, Y (2008). "Delayed gastric emptying: the state of the highest level of evidence". J Hepatobiliary Pancreat Surg. 15 (3): 262–9. doi:10.1007/s00534-007-1304-8. PMID 18535763.
- Bassi, C; Dervenis, C; Butturini, G; Fingerhut, A; Yeo, C; Izbicki, J; Neoptolemos, J; Sarr, M; Traverso, W; Buchler, M (2005). "Postoperative pancreatic fistula: an international study group (ISGPF) definition". Surgery. 138 (1): 8–13. doi:10.1016/j.surg.2005.05.001. PMID 16003309.
- Cullen, JJ; Sarr, MG; Ilstrup, DM (1994). "Pancreatic anastomotic leak after pancreaticoduodenectomy: incidence, significance, and management". Am J Surg. 168 (4): 295–8. doi:10.1016/s0002-9610(05)80151-5. PMID 7524375.
- Tan, Winson Jianhong; Kow, Alfred Wei Chieh; Liau, Kui Hin (August 2011). "Moving towards the New International Study Group for Pancreatic Surgery (ISGPS) definitions in pancreaticoduodenectomy: a comparison between the old and new". HPB. 13 (8): 566–572. doi:10.1111/j.1477-2574.2011.00336.x. ISSN 1365-182X. PMC 3163279. PMID 21762300.
- Sugawara, Kotaro; Kawaguchi, Yoshikuni; Nomura, Yukihiro; Suka, Yusuke; Kawasaki, Keishi; Uemura, Yukari; Koike, Daisuke; Nagai, Motoki; Furuya, Takatoshi (2017-11-08). "Perioperative Factors Predicting Prolonged Postoperative Ileus After Major Abdominal Surgery". Journal of Gastrointestinal Surgery. 22 (3): 508–515. doi:10.1007/s11605-017-3622-8. ISSN 1873-4626. PMID 29119528.
- Livingston, E. H.; Passaro, E. P. (January 1990). "Postoperative ileus". Digestive Diseases and Sciences. 35 (1): 121–132. doi:10.1007/bf01537233. ISSN 0163-2116. PMID 2403907.
- Vather, Ryash; Bissett, Ian (May 2013). "Management of prolonged post-operative ileus: evidence-based recommendations". ANZ Journal of Surgery. 83 (5): 319–324. doi:10.1111/ans.12102. ISSN 1445-2197. PMID 23418987.
- synd/3492 at Who Named It?
External links
- Toronto Whipple Clinical Pathway Education App - Open access App for patient and caregiver education
- The Toronto Video Atlas of Liver, Pancreas and Transplant Surgery – Video of Whipple procedure
- The Toronto Video Atlas of Liver, Pancreas and Transplant Surgery Patient Education Module – Patient and Family Education video for the Whipple procedure
- " Whipple pancreaticoduodenectomy: a historical comment Adrian O'Sullivan – The original description of Whipple's operation together with a modern commentary