Bicornuate uterus
A bicornuate uterus or bicornate uterus (from the Latin cornū, meaning "horn"), is a type of mullerian anomaly in the human uterus, where there is a deep indentation at the fundus (top) of the uterus.
| Bicornuate uterus | |
|---|---|
| Other names | bicornate uterus |
 | |
| A human bicornuate uterus | |
| Specialty | Gynaecology |
Pathophysiology
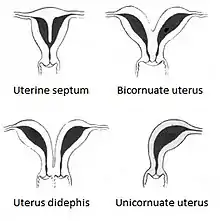
A bicornuate uterus develops during embryogenesis. It occurs when the proximal (upper) portion of the paramesonephric ducts does not fuse, but the distal portion that develops into the lower uterine segment, cervix, and upper vagina fuses normally.[1]
Diagnosis

Diagnosis of bicornuate uterus typically involves imaging of the uterus with 2D or 3D ultrasound, hysterosalpingography, or magnetic resonance imaging (MRI). On imaging, a bicornuate uterus can be distinguished from a septate uterus by the angle between the cornua (intercornual angle): less than 75 degrees in a septate uterus, and greater than 105 degrees in a bicornuate uterus. Measuring the depth of the cleft between the cornua (fundal cleft) may also assist in diagnosis; a cleft of over 1 centimetre (0.39 in) is indicative of bicornuate uterus.[2]
Classification
Bicornuate uterus is typically classified based on whether or not the division extends to the external cervical os. Bicornuate uteri with a division above the os are called bicornuate unicollis and those with a divided os are called bicornuate bicollis.[2] There is a continuous range of the degree and location of the fusion of the paramesonephric ducts, and existence of a spectrum, rather than a fixed number of types corresponding to strict medical definitions. Two processes that occur during the embryonic development of the paramesonephric ducts — fusion and reabsorption — can be affected to different degrees.[3]
There is also a hybrid bicornuate uterus: External fundal depressions of variable depths associated with a septate uterus can be seen by laparoscopy, indicating the coexistence of the two anomalies. These cases are candidates for hysteroscopic metroplasty under appropriate sonographic and/or laparoscopic monitoring.[4]
An obstructed bicornuate uterus showing uni or bilateral obstruction might also be possible. The unilateral obstruction is more difficult to diagnose than the bilateral obstructive. A delay in the diagnosis can be problematic and compromise the reproductive abilities of those cases.[5]
Treatment
Bicornuate uterus typically requires no treatment.[1] In those who do need treatment, metroplasty is the surgical correction of choice.[2] People who have recurrent miscarriage with no other explanation may benefit from surgery.[6]
Epidemiology
The occurrence of all types of paramesonephric duct abnormalities in women is estimated around 0.4%.[7] A bicornuate uterus is estimated to occur in 0.1–0.6% of women in the US.[8] It is possible that this figure is an underestimate, since subtle abnormalities often go undetected. Some intersex individuals whose external genitalia are perceived as being male may nonetheless have a variably shaped uterus. Women exposed in utero to diethylstilbestrol (DES) are at risk for this abnormality.
In pregnancy
A bicornuate uterus is an indication for increased surveillance of a pregnancy, though most people with a bicornuate uterus are able to have healthy pregnancies.[1] People with a bicornuate uterus are at an increased risk of recurrent miscarriage,[2][9] preterm birth,[2][10] malpresentation,[2][11] disruptions to fetal growth,[12] premature rupture of membranes, placenta previa and retained placenta (which can lead to postpartum hemorrhage).[13] This is due to the distortion of the normal shape of the uterus, distortion of the cervix leading to cervical insufficiency, or under-vascularization of the endometrium as the pregnancy requires more blood supply. In some cases, the nonpregnant horn can rupture during labor, necessitating emergency surgery.[13]
Fetuses developing in bicornuate uteri are more likely to present breech or transverse, with the fetal head in one horn and the feet in the other. This will often necessitate cesarean delivery. If the fetus is vertex (head down), the two horns may not contract in coordination, or the horn that does not contain the pregnancy may interfere with contractions and descent of the fetus, causing obstructed labor.[13]
Effect on intrauterine device usage
Usage of intrauterine device (IUD) with copper requires one IUD in each horn to be effective in case of bicornuate uterus. The same practice is generally applied when using IUD with progestogen due to lack of evidence of efficacy with only one IUD.[14]Evidence is lacking regarding progestogen IUD usage for menorrhagia in bicornuate uterus, but a case report showed good effect with a single IUD.[15]
References
- Bauman, D. (2013). "Pediatric & Adolescent Gynecology". CURRENT Diagnosis & Treatment: Obstetrics & Gynecology. McGraw-Hill.
- Cunningham F, Leveno KJ, Bloom SL, Dashe JS, Hoffman BL, Casey BM, Spong CY (eds.). "Congenital Genitourinary Abnormalities". Williams Obstetrics (25 ed.). McGraw-Hill.
- Acién P, Acién M, Sánchez-Ferrer ML (2008). "Müllerian anomalies "without a classification": from the didelphys-unicollis uterus to the bicervical uterus with or without septate vagina". Fertil. Steril. 91 (6): 2369–75. doi:10.1016/j.fertnstert.2008.01.079. PMID 18367185.
- El Saman AM, Shahin AY, Nasr A, Tawfik RM, Saadeldeen HS, Othman ER, Habib DM, Abdel-Aleem MA (Nov 2012). "Hybrid septate uterus, coexistence of bicornuate and septate varieties: a genuine report". J Obstet Gynaecol Res. 38 (11): 1308–14. doi:10.1111/j.1447-0756.2012.01866.x. PMID 22612567. S2CID 6177612.CS1 maint: multiple names: authors list (link)
- El Saman AM, Nasr A, Tawfik RM, Saadeldeen HS (Aug 2011). "Müllerian duct anomalies: successful endoscopic management of a hybrid bicornuate/septate variety". J Pediatr Adolesc Gynecol. 24 (4): e89–92. doi:10.1016/j.jpag.2011.02.013. PMID 21514191.CS1 maint: multiple names: authors list (link)
- Hoffman BL, Schorge JO, Bradshaw KD, Halvorson LM, Schaffer JI, Corton MM (eds.). "Anatomic Disorders". Williams Gynecology (3 ed.).
- Byrne J, Nussbaum-Blask A, Taylor WS, et al. (2000). "Prevalence of Müllerian duct anomalies detected at ultrasound". Am. J. Med. Genet. 94 (1): 9–12. doi:10.1002/1096-8628(20000904)94:1<9::AID-AJMG3>3.0.CO;2-H. PMID 10982475.
- "Bicornuate Uterus - an overview | ScienceDirect Topics". www.sciencedirect.com. Retrieved 2021-01-04.
- Rackow BW, Arici A (2007). "Reproductive performance of women with müllerian anomalies". Curr. Opin. Obstet. Gynecol. 19 (3): 229–37. doi:10.1097/GCO.0b013e32814b0649. PMID 17495638. S2CID 5476966.
- Airoldi J, Berghella V, Sehdev H, Ludmir J (2005). "Transvaginal ultrasonography of the cervix to predict preterm birth in women with uterine anomalies". Obstet Gynecol. 106 (3): 553–6. doi:10.1097/01.AOG.0000173987.59595.e2. PMID 16135586. S2CID 22903707.
- Heinonen PK, Saarikoski S, Pystynen P (1982). "Reproductive performance of women with uterine anomalies. An evaluation of 182 cases". Acta Obstet Gynecol Scand. 61 (2): 157–62. doi:10.3109/00016348209156548. PMID 7113692. S2CID 72723061.
- Martı́Nez-Frı́As, María Luisa; Bermejo, Eva; Rodrı́Guez-Pinilla, Elvira; Frı́As, Jaime Luis (1998). "Congenital Anomalies in the Offspring of Mothers with a Bicornuate Uterus". Pediatrics. 101 (4): e10. doi:10.1542/peds.101.4.e10. PMID 9521976.
- Pascali, Dante (2014). "Uterus and Vagina". Oxorn-Foote Human Labor & Birth, 6e.
- Amies Oelschlager, Anne-Marie; Debiec, Kate; Micks, Elizabeth; Prager, Sarah (2013). "Use of the Levonorgestrel Intrauterine System in Adolescents With Known Uterine Didelphys or Unicornuate Uterus". Journal of Pediatric and Adolescent Gynecology. 26 (2): e58. doi:10.1016/j.jpag.2013.01.029. ISSN 1083-3188.
- Acharya GP, Mills AM (July 1998). "Successful management of intractable menorrhagia with a levonorgestrel-releasing intrauterine device, in a woman with a bicornuate uterus". J Obstet Gynaecol. 18 (4): 392–3. doi:10.1080/01443619867263. PMID 15512123.