Developmental language disorder
Developmental language disorder (DLD) is identified when a child has problems with language development that continue into school age and beyond. The language problems have a significant impact on everyday social interactions or educational progress, and occur in the absence of autism spectrum disorder, intellectual disability or a known biomedical condition. The most obvious problems are difficulties in using words and sentences to express meanings, but for many children, understanding of language (receptive language) is also a challenge, although this may not be evident unless the child is given a formal assessment.
| Developmental language disorder | |
|---|---|
| Specialty | Neurology |
Classification
Terminology
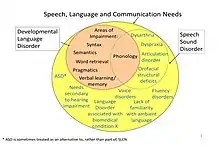
The term developmental language disorder (DLD) was endorsed in a consensus study involving a panel of experts (CATALISE Consortium) in 2017.[1] The study was conducted in response to concerns that a wide range of terminology was used in this area, with the consequence that there was poor communication, lack of public recognition, and in some cases children were denied access to services. Developmental language disorder is a subset of language disorder, which is itself a subset of the broader category of speech, language and communication needs (SLCN).
The terminology for children’s language disorders has been extremely wide-ranging and confusing, with many labels that have overlapping but not necessarily identical meanings.[2] In part this confusion reflected uncertainty about the boundaries of DLD, and the existence of different subtypes. Historically, the terms ‘’developmental dysphasia’’ or ‘’developmental aphasia’’ were used to describe children with the clinical picture of DLD.[3] These terms have, however, largely been abandoned, as they suggest parallels with adult acquired aphasia. This is misleading, as DLD is not caused by brain damage.[4]
Although the term DLD has been used for many years, it has been less common than the term specific language impairment (SLI),[2] which has been widely adopted, especially in North America.[5] The definition of SLI overlaps with DLD, but was rejected by the CATALISE panel because it was seen as overly restrictive in implying that the child had relatively pure problems with language in the absence of any other impairments. Children with such selective problems are relatively rare, and there is no evidence that they respond differently to intervention, or have different causal factors, from other children with language problems.[6]
In the UK education system the term speech, language and communication needs (SLCN) is widely used, but this is far broader than DLD, and includes children with speech, language and social communication difficulties arising from a wide range of causes.[7]
The question of whether to refer to children's language problems as ‘disorder’ was a topic of debate among the CATALISE consortium, but the conclusion was that ‘disorder’ conveyed the serious nature and potential consequences of persistent language deficits. It is also parallel with other neurodevelopmental conditions and consistent with diagnostic frameworks such as DSM-5 and ICD-11.[1] Where there are milder or more transient difficulties, language difficulties may be a more appropriate term.
Types of language difficulty
DLD can affect a range of areas of language and the degree of impairment in different areas of language can vary from child to child.[8] However, although there have been attempts to define different subtypes, these have not generally resulted in robust categories.[9] The recommendation of the CATALISE panel was that the specific areas of impairment should be assessed and documented for individual children, while recognizing that different children might have different combinations of problems. The areas which can be affected are:
- Grammar – This involves the ability to combine words into grammatically correct sentences (syntax) and to combine parts of words together (morphology) such as adding grammatical endings to verbs like -ing or -ed or to add prefixes and suffixes like dis- or -ation. For instance, a child may say 'me jump here', instead of 'I jumped here'.[10] Comprehension of sentences can also be affected. For instance, there may be difficulty understanding meaning expressed by word order, and so confusion about what is blue in a sentence like 'the pencil on the shoe is blue',[11] and a tendency to use general knowledge rather than linguistic cues to meaning,[12] or problems in interpreting grammatical markers of number or tense.[13]
- Semantics – This refers to children’s ability to understand the meaning of words and how meanings are expressed by combining words together. Children with DLD often have limited vocabulary and may make heavy use of a small set of words with rather general meanings.[14] As children with developmental language disorder get older, they may have a hard time understanding that some words have multiple meanings, for example the word “cold,” which can mean a low temperature, a sickness, or being unfriendly.[15][14]
- Word finding – Children with word finding difficulties may know a word, but have difficulty accessing it for production[16] – similar to the tip of the tongue phenomenon.
- Pragmatics – Pragmatics refers to the ability to select the appropriate message, or interpret what others say, in relation to context. Pragmatic difficulties can give an impression of oddity, with the content of language not fitting the environmental or social context; comprehension may be over-literal; the child may chatter incessantly, be poor at turn-taking in conversation and maintaining a topic[17]
- Discourse – Discourse refers to a level of organization of language beyond the sentence. Child with limitations in this domain may have limited ability to tell a story or describe a set of events in a logical sequence[18]
- Verbal memory and learning – Problems with remembering words or sentences can affect both the learning of new vocabulary,[19] and the understanding of long or complex sentences.[20] Young children with DLD may say their first words later than other children. It may also take children with DLD longer to learn and remember novel words.[15]
- Phonology – Phonology is the branch of linguistics concerned with the way sounds are combined together in words. Children with difficulties with phonology may fail to distinguish between certain speech sounds, such as 't' and 'k', so that 'cake' is produced as 'tate'. Such difficulties are not unusual as part of typical development in toddlers, but they would usually resolve by the time children are 4–5 years old.[21] Difficulties with producing some speech sounds accurately may reduce intelligibility of speech.[22] In addition, more subtle difficulties in recognising specific sounds in words (phonological awareness) can lead to literacy difficulties.[23]
Relationship with speech disorders
Speech is the act of articulating sounds, and this can be impaired for all kinds of reasons – a structural problem such as cleft lip and cleft palate, a neurological problem affecting motor control of the speech apparatus dysarthria, or inability to perceive distinctions between sounds because of hearing loss. Some distortions of speech sounds, such as a lisp, are commonly seen in young children. These misarticulations should not be confused with language problems, which involve the ability to select and combine linguistic elements to express meanings, and the ability to comprehend meanings.
Although speech disorders can be distinguished from language disorders, they can also co-occur.[24] When a child fails to produce distinctions between speech sounds for no obvious reason, this is typically regarded as a language problem affecting the learning of phonological contrasts. The classification of and terminology for disorders of speech sound production is a subject of considerable debate.[25] In practice, even for those with specialist skills, it is not always easy to distinguish between phonological disorders and other types of speech production problem. Speech sound disorder (SSD) is any problem with speech production arising from any cause.[26]
Speech sound disorders of unknown cause that are not accompanied by other language problems are a relatively common reason for young children to be referred to speech-language therapy (speech-language pathology).[27] These often resolve by around 4–5 years of age with specialist intervention,[28] and so would not meet criteria for DLD. Where such problems continue beyond five years of age, they are usually accompanied by problems in broader language domains and have a poorer prognosis,[29] so a diagnosis of DLD with SSD is then appropriate.
Relationship with other neurodevelopmental disorders
DLD often co-occurs with milder neurodevelopmental disorders of unknown origin, such as attention-deficit hyperactivity disorder, developmental dyslexia or developmental co-ordination disorder.[6] These do not preclude a diagnosis of DLD, but should be noted as co-occurring conditions.
Risk factors
It is generally accepted that DLD is strongly influenced by genetic factors.[30] The best evidence comes from the twin study method. Two twins growing up together are exposed to the same home environment, yet may differ radically in their language skills. Such different outcomes are, however, much more common in fraternal (non-identical) twins, who are genetically different. Identical twins share the same genes and tend to be much more similar in language ability. There can be some variation in the severity and persistence of DLD in identical twins, indicating that non-genetic factors affect the course of disorder, but it is unusual to find a child with DLD who has an identical twin with typical language.[31]
There was considerable excitement when a large, multigenerational family with a high rate of DLD were found to have a mutation of the FOXP2 gene just in the affected family members.[32] However, subsequent studies have found that, though DLD runs in families, it is not usually caused by a mutation in FOXP2 or another specific gene.[33] Current evidence suggests that there are many different genes that can influence language learning, and DLD results when a child inherits a particularly detrimental combination of risk factors, each of which may have only a small effect.[30] Nevertheless, study of the mode of action of the FOXP2 gene has helped identify other common genetic variants involved in the same neural pathways that may play a part in causing DLD.[34]
Language disorders are associated with aspects of home environment, and it is often assumed that this is a causal link, with poor language stimulation leading to weak language skills. Twin studies, however, show that two children in the same home environment can have very different language outcomes, suggesting we should consider other explanations for the link. Children with DLD often grow up into adults who have relatively low educational attainments,[35] and their children may share a genetic risk for language disorder.[2]
One non-genetic factor that is known to have a specific impact on language development is being a younger sibling in a large family.[36]
Associated factors
It has long been noted that males are more affected by DLD than females, with a sex ratio of affected males: females around 3 or 4:1.[37] However, the sex difference is much less striking in epidemiological samples, suggesting that similar problems may exist in females but are less likely to be detected.[38] The reason for the sex difference is not well understood.
Poor motor skills are commonly found in children with DLD.[39] Standardized measures of motor ability confirm that children with DLD exhibit deficits in fine and gross motor skill, both simple and complex. These difficulties also extend to speech-motor ability, particularly with the control of their articulatory movements. Children with DLD have difficulty with motor sequence learning and may show deficits in other procedural motor processes as well.[40]
Brain scans do not usually reveal any obvious abnormalities in children with DLD, although quantitative comparisons have found differences in brain size or relative proportions of white or grey matter in specific regions. In some cases, unusual brain gyri are found. To date, no consistent 'neural signature' for DLD has been found, although some studies have noted evidence for involvement of subcortical systems.[41] Differences in the brains of children with DLD vs typically developing children are subtle and may overlap with atypical patterns seen in other neurodevelopmental disorders.[42]
Diagnosis
DLD is defined purely in behavioural terms: there is no biological test. There are three points that need to be met for a diagnosis of DLD:[1]
- The child has language difficulties that create obstacles to communication or learning in everyday life,
- The child's language problems are unlikely to resolve by five years of age, and
- The problems are not associated with a known biomedical condition such as brain injury, neurodegenerative conditions, genetic conditions or chromosome disorders such as Down syndrome, sensorineural hearing loss, or autism spectrum disorder or intellectual disability.
For research and epidemiological purposes, specific cutoffs on language assessments have been used to document the first criterion. Tomblin et al.[43] proposed the EpiSLI criterion, based on five composite scores representing performance in three domains of language (vocabulary, grammar, and narration) and two modalities (comprehension and production). Children scoring in the lowest 10% on two or more composite scores are identified as having language disorder.
The second criterion, persistence of language problems, can be difficult to judge in a young child, but longitudinal studies have shown that difficulties are less likely to resolve for children who have poor language comprehension, rather than difficulties confined to expressive language.[1] In addition, children with isolated difficulties in just one of the areas noted under 'subtypes' tend to make better progress than those whose language is impaired in several areas.[29]
The third criterion specifies that DLD is used for children whose language disorder is not part of another biomedical condition, such as a genetic syndrome, a sensorineural hearing loss, neurological disease, autism spectrum disorder or intellectual disability – these were termed 'differentiating conditions' by the CATALISE panel.[1] Language disorders occurring with these conditions need to be assessed and children offered appropriate intervention, but a terminological distinction is made so that these cases would be diagnosed as language disorder associated with the main diagnosis being specified: e.g. "language disorder associated with autism spectrum disorder." The reasoning behind these diagnostic distinctions is discussed further by Bishop (2017).[44]
Benchmarks for children with Developmental Language Disorder
Common red flags at one year of age
- No reaction to sound
- No babbling
- Difficulty feeding
- No imitation
- Limited use of gestures
At two years of age
- Makes minimal attempts to communicate with gestures or words
- Has not spoken their first words
- Difficulty following simple directions
- Inconsistent response to "no"
At three years of age
- Limited use of speech
- Incomprehensible speech
- Limited understanding of simple questions
- Difficulty naming objects
- Frustration related to communication
At four years of age
- Uses only 3 word phrases
- Speech is not understandable to parents
- Takes a long time to understand others
- Difficulty asking questions and finding words to express thoughts
At five years of age
- Speaks only in simple sentences
- Speech is not understandable to teachers
- Difficulty answering questions
- Difficulty with complex directions
- Difficulty telling stories
- Difficulty with peer interactions [45]
Assessment
Assessment will usually include an interview with the child’s caregiver, observation of the child in an unstructured setting, a hearing test, and standardized tests of language.[46] There is a wide range of language assessments in English. Some are restricted for use by experts in speech-language pathology: speech and language therapists (SaLTs/SLTs) in the UK, speech-language pathologists (SLPs) in the US and Australia. A commonly used test battery for diagnosis of DLD is the Clinical Evaluation of Language Fundamentals (CELF). Assessments that can be completed by a parent or teacher can be useful to identify children who may require more in-depth evaluation. The Children’s Communication Checklist (CCC–2) is a parent questionnaire suitable for assessing everyday use of language in children aged four years and above who can speak in sentences. Informal assessments, such as language samples, are often used by speech-language therapists/pathologists to complement formal testing and give an indication of the child's language in a more naturalistic context. A language sample may be of a conversation or narrative retell. In a narrative language sample, an adult may tell the child a story using a wordless picture book (e.g. Frog Where Are You?, Mayer, 1969), then ask the child to use the pictures and tell the story back. Language samples can be transcribed using computer software such as the Systematic Analysis of Language Software, and then analyzed for a range of features: e.g., the grammatical complexity of the child's utterances, whether the child introduces characters to their story or jumps right in, whether the events follow a logical order, and whether the narrative includes a main idea or theme and supporting details.
Treatment
Treatment is usually carried out by speech and language therapists/pathologists, who use a wide range of techniques to stimulate language learning.[47] In the past, there was a vogue for drilling children in grammatical exercises, using imitation and elicitation, but such methods fell into disuse when it became apparent that there was little generalisation to everyday situations. Contemporary approaches to enhancing development of language structure, for younger children at least, are more likely to adopt 'milieu' methods, in which the intervention is interwoven into natural episodes of communication, and the therapist builds on the child's utterances, rather than dictating what will be talked about. Interventions for older children, may be more explicit, telling the children what areas are being targeted and giving explanations regarding the rules and structures they are learning, often with visual supports.[48][49]
In addition, there has been a move away from a focus solely on grammar and phonology toward interventions that develop children's social use of language, often working in small groups that may include typically developing as well as language-impaired peers.[50]
Another way in contemporary remediation differ from the past is that parents are more likely to be directly involved, but this approach is largely used with preschool children, rather than those whose problems persist into school age.[51][52]
For school-aged children, teachers are increasingly involved in intervention, either in collaboration with speech and language therapists/pathologists, or as the main agents of delivery of the intervention. Evidence for the benefits of a collaborative approach is emerging,[53] but the benefits of asking education staff to be the main deliverers of SLT intervention (the “consultative” approach) are unclear.[54] When SLT intervention is delivered indirectly by trained SLT assistants, however, there are indications that this can be effective.[55]
In this field, randomized controlled trial methodology has not been widely used, and this makes it difficult to assess clinical efficacy with confidence. Children's language will tend to improve over time, and without controlled studies, it can be hard to know how much of observed change is down to a specific treatment. There is, however, increasing evidence that direct 1:1 intervention with an SLT/P can be effective for improving vocabulary and expressive language.[56] There have been few studies of interventions that target receptive language,[57] though some positive outcomes have been reported.[58][59][60]
How to help a child with Developmental Language Disorder
- Talk to the child often to help them learn new words.
- Read to them every day. Point out words you see.
- Point to signs in the grocery store, at school, and outside.
- Speak to the child in the language you know best.
- Listen and answer when the child talks.
- Get the child to ask you questions.
- Give the child time to answer questions.
- Keep them in school. Children who are school-refusers have poorer language skills overall, and a higher incidence of language impairments[61]
Outcome
Longitudinal studies indicate that problems are largely resolved by five years of age in around 40% of four-year-olds with early language delays who have no other presenting risk factors.[29] However, for children who still have significant language difficulties at school entry, reading problems are common, even for children who receive specialist help,[62] and educational attainments are typically poor.[63] Poor outcomes are most common in cases where comprehension as well as expressive language is affected.[64] There is also evidence that scores on tests of nonverbal ability of children with DLD decrease over the course of development.[65]
DLD is associated with an elevated risk of social, emotional and mental health concerns.[66] For instance, in a UK survey, 64% of a sample of 11-year-olds with DLD scored above a clinical threshold on a questionnaire for psychiatric difficulties, and 36% were regularly bullied, compared with 12% of comparison children.[67] In the longer-term, studies of adult outcomes of children with DLD have found elevated rates of unemployment, social isolation and psychiatric disorder among those with early comprehension difficulties.[68] However, better outcomes are found for children who have milder difficulties and do not require special educational provision.[69]
Prevalence
Epidemiological surveys, in the US[70] and the UK[38] converge in estimating the prevalence of DLD in five-year-olds at around 7%. Therefore, the prevalence is one in every 15 children. By these statistics, in a classroom of 30 students, 2 would have DLD.[15] In research by Tomblin et al. prevalence of [DLD] in racial/ethnic groups was highest in Native Americans, with African Americans being the next highest, followed by Hispanics, and then Whites.[71] No students of Asian descent presented with [DLD]; however, other research does indicate that [DLD] is present in children of Asian descent).
Research
Much research has focused on trying to identify what makes language learning so hard for some children.[72] A major divide is between theories that attribute the difficulties to a low-level problem with auditory temporal processing, and those that propose there is a deficit in a specialised language-learning system.[73][74] Other accounts emphasise deficits in specific aspects of learning and memory.[75][76] It can be difficult to choose between theories because they do not always make distinctive predictions, and there is considerable heterogeneity among children with DLD. It has also been suggested that DLD may only arise when more than one underlying deficit is present.[77]
Developmental learning disorder in adults
Relatively little research has been conducted to test the outcomes of DLD in adults. In a study comparing 17 men with DLD to their non language disordered siblings, researchers found that The DLD men had normal intelligence with higher performance IQ than verbal IQ. The participants still exhibited a severe and persisting language disorder, severe literacy impairments and significant deficits in theory of mind and phonological processing. Within the DLD cohort higher childhood intelligence and language were associated with superior cognitive and language ability at final adult outcome. In their mid-thirties, the DLD cohort had significantly worse social adaptation (with prolonged unemployment and a paucity of close friendships and love relationships) compared with both their siblings and NCDS controls. Self-reports showed a higher rate of schizotypal features but not affective disorder. Four DLD adults had serious mental health problems (two had developed schizophrenia).[78]
See also
References
- Bishop, Dorothy V.M.; Snowling, Margaret J.; Thompson, Paul A.; Greenhalgh, Trisha (October 2017). "Phase 2 of CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology". Journal of Child Psychology and Psychiatry. 58 (10): 1068–1080. doi:10.1111/jcpp.12721. PMC 5638113. PMID 28369935.
- Bishop, D. V. M. (July 2014). "Ten questions about terminology for children with unexplained language problems". International Journal of Language & Communication Disorders. 49 (4): 381–415. doi:10.1111/1460-6984.12101. PMC 4314704. PMID 25142090.
- Ingram, T. T. S.; Reid, J. F. (June 1956). "Developmental Aphasia Observed in a Department of Child Psychiatry". Archives of Disease in Childhood. 31 (157): 161–172. doi:10.1136/adc.31.157.161. PMC 2011959. PMID 13328151.
- Rapin, Isabelle (September 1996). "Practitioner Review: Developmental Language Disorders: A Clinical Update". Journal of Child Psychology and Psychiatry. 37 (6): 643–655. doi:10.1111/j.1469-7610.1996.tb01456.x. PMID 8894945.
- Leonard, Laurence B. (April 1991). "Specific Language Impairment as a Clinical Category". Language, Speech, and Hearing Services in Schools. 22 (2): 66–68. doi:10.1044/0161-1461.2202.66.
- Bishop, D. V. M.; Snowling, Margaret J.; Thompson, Paul A.; Greenhalgh, Trisha; Schiller, Niels O. (8 July 2016). "CATALISE: A Multinational and Multidisciplinary Delphi Consensus Study. Identifying Language Impairments in Children". PLOS ONE. 11 (7): e0158753. Bibcode:2016PLoSO..1158753B. doi:10.1371/journal.pone.0158753. PMC 4938414. PMID 27392128.
- Bercow, J. (2008). The Bercow Report: A Review of Services for Children and Young People (0-19) with Speech, Language and Communication Needs Archived 2012-10-16 at the Wayback Machine. Nottingham: DCSF Publications. However, the UK special educational needs system uses SLCN in a manner which is more similar to DLD.
- van Weerdenburg, Marjolijn; Verhoeven, Ludo; van Balkom, Hans (February 2006). "Towards a typology of specific language impairment". Journal of Child Psychology and Psychiatry. 47 (2): 176–189. doi:10.1111/j.1469-7610.2005.01454.x. PMID 16423149.
- Conti-Ramsden, Gina; Botting, Nicola (1 October 1999). "Classification of Children With Specific Language Impairment". Journal of Speech, Language, and Hearing Research. 42 (5): 1195–1204. doi:10.1044/jslhr.4205.1195. PMID 10515515.
- Leonard, L. B. (2014). Children with specific language impairment, 2nd edition. Cambridge, MA: MIT Press.
- Bishop, D. V. M. (January 1982). "Comprehension of Spoken, Written and Signed Sentences in Childhood Language Disorders". Journal of Child Psychology and Psychiatry. 23 (1): 1–20. doi:10.1111/j.1469-7610.1982.tb00045.x. PMID 6174536.
- Paul, Rhea (June 1990). "Comprehension strategies: Interactions between world knowledge and the development of sentence comprehension". Topics in Language Disorders. 10 (3): 63–75. doi:10.1097/00011363-199006000-00007. S2CID 144481133.
- Leonard, Laurence B.; Deevy, Patricia (2010). "Tense and Aspect in Sentence Interpretation by Children with Specific Language Impairment". Journal of Child Language. 37 (2): 395–418. doi:10.1017/S0305000909990018. PMC 3640588. PMID 19698206.
- Rice, Mabel L.; Bode, John V. (1993). "GAPS in the verb lexicons of children with specific language impairment". First Language. 13 (37): 113–131. doi:10.1177/014272379301303707. S2CID 144261715.
- Kuiack, Alyssa; Archibald, Lisa (9 July 2019). "Developmental Language Disorder: The Childhood Condition We Need to Start Talking About". Frontiers for Young Minds. 7. doi:10.3389/frym.2019.00094.
- German, Diane J. (November 1992). "Word-finding intervention for children and adolescents". Topics in Language Disorders. 13 (1): 33–50. doi:10.1097/00011363-199211000-00006. S2CID 143899095.
- Adams, Catherine (January 2001). "Clinical diagnostic and intervention studies of children with semantic—pragmatic language disorder". International Journal of Language & Communication Disorders. 36 (3): 289–305. doi:10.1080/lcd.36.3.289.305.
- Van der Lely, Heather K. J. (1 February 1997). "Narrative discourse in Grammatical specific language impaired children: a modular language deficit?". Journal of Child Language. 24 (1): 221–256. doi:10.1017/s0305000996002966. PMID 9154015.
- Gathercole, Susan E. (25 July 2016). "Word learning in language-impaired children". Child Language Teaching and Therapy. 9 (3): 187–199. doi:10.1177/026565909300900302. S2CID 145471438.
- Montgomery, James W. (May 2002). "Information Processing and Language Comprehension in Children with Specific Language Impairment". Topics in Language Disorders. 22 (3): 62–84. doi:10.1097/00011363-200205000-00007.
- Rvachew, S., & Brosseau-Lapre, F. (2012). Developmental Phonological Disorders: Foundations of clinical Practice: Plural Publishing Inc.
- Klein, Edward S.; Flint, Cari B. (July 2006). "Measurement of Intelligibility in Disordered Speech". Language, Speech, and Hearing Services in Schools. 37 (3): 191–199. doi:10.1044/0161-1461(2006/021). PMID 16837442.
- Kamhi, Alan G.; Catts, Hugh W.; Mauer, Daria; Apel, Kenn; Gentry, Betholyn F. (1 August 1988). "Phonological and Spatial Processing Abilities in Language- and Reading-Impaired Children". Journal of Speech and Hearing Disorders. 53 (3): 316–327. doi:10.1044/jshd.5303.316. PMID 3398484.
- Shriberg, Lawrence D.; Tomblin, J. Bruce; McSweeny, Jane L. (1 December 1999). "Prevalence of Speech Delay in 6-Year-Old Children and Comorbidity With Language Impairment". Journal of Speech, Language, and Hearing Research. 42 (6): 1461–1481. doi:10.1044/jslhr.4206.1461. PMID 10599627.
- Waring, R.; Knight, R. (January 2013). "How should children with speech sound disorders be classified? A review and critical evaluation of current classification systems" (PDF). International Journal of Language & Communication Disorders. 48 (1): 25–40. doi:10.1111/j.1460-6984.2012.00195.x. PMID 23317382.
- Bowen, C. (2015). Children's Speech Sound Disorders (2nd ed.). Oxford: Wiley-Blackwell.
- Broomfield, Jan; Dodd, Barbara (January 2004). "Children with speech and language disability: caseload characteristics". International Journal of Language & Communication Disorders. 39 (3): 303–324. doi:10.1080/13682820310001625589. PMID 15204443.
- Law, James; Garrett, Zoe; Nye, Chad (21 July 2003). "Speech and language therapy interventions for children with primary speech and language delay or disorder". Cochrane Database of Systematic Reviews (3): CD004110. doi:10.1002/14651858.CD004110. PMID 12918003.
- Bishop, D. V. M.; Edmundson, A. (1 May 1987). "Language-Impaired 4-Year-Olds". Journal of Speech and Hearing Disorders. 52 (2): 156–173. doi:10.1044/jshd.5202.156. PMID 3573746.
- Bishop, Dorothy V M (October 2006). "What Causes Specific Language Impairment in Children?". Current Directions in Psychological Science. 15 (5): 217–221. doi:10.1111/j.1467-8721.2006.00439.x. PMC 2582396. PMID 19009045.
- Bishop, D. V. M.; North, T.; Donlan, C. (12 November 2008). "Genetic Basis of Specific Language Impairment: Evidence from a Twin Study". Developmental Medicine & Child Neurology. 37 (1): 56–71. doi:10.1111/j.1469-8749.1995.tb11932.x. PMID 7828787. S2CID 21594745.
- Fisher, Simon E.; Vargha-Khadem, Faraneh; Watkins, Kate E.; Monaco, Anthony P.; Pembrey, Marcus E. (February 1998). "Localisation of a gene implicated in a severe speech and language disorder". Nature Genetics. 18 (2): 168–170. doi:10.1038/ng0298-168. hdl:11858/00-001M-0000-0012-CBD9-5. PMID 9462748. S2CID 3190318.
- Fisher, S (September 2006). "Tangled webs: Tracing the connections between genes and cognition". Cognition. 101 (2): 270–297. doi:10.1016/j.cognition.2006.04.004. hdl:11858/00-001M-0000-0012-CB28-2. PMID 16764847. S2CID 10595435.
- Fisher, Simon E.; Scharff, Constance (April 2009). "FOXP2 as a molecular window into speech and language". Trends in Genetics. 25 (4): 166–177. doi:10.1016/j.tig.2009.03.002. PMID 19304338.
- Whitehouse, Andrew J O; Watt, Helen J; Line, E A; Bishop, Dorothy V M (2009). "Adult psychosocial outcomes of children with specific language impairment, pragmatic language impairment and autism". International Journal of Language & Communication Disorders. 44 (4): 511–528. doi:10.1080/13682820802708098. PMC 2835860. PMID 19340628.
- Fundudis, T., Kolvin, I., & Garside, R. (1979). Speech Retarded and Deaf Children: Their Psychological Development. London: Academic Press.
- Robinson, Roger J. (12 November 2008). "Causes and Associations of Severe and Persistent Specific Speech and Language Disorders in Children". Developmental Medicine & Child Neurology. 33 (11): 943–962. doi:10.1111/j.1469-8749.1991.tb14811.x. PMID 1720749. S2CID 7412606.
- Norbury, Courtenay Frazier; Gooch, Debbie; Wray, Charlotte; Baird, Gillian; Charman, Tony; Simonoff, Emily; Vamvakas, George; Pickles, Andrew (November 2016). "The impact of nonverbal ability on prevalence and clinical presentation of language disorder: evidence from a population study". Journal of Child Psychology and Psychiatry. 57 (11): 1247–1257. doi:10.1111/jcpp.12573. PMC 5082564. PMID 27184709.
- Hill, Elisabeth L. (January 2001). "Non-specific nature of specific language impairment: a review of the literature with regard to concomitant motor impairments" (PDF). International Journal of Language & Communication Disorders. 36 (2): 149–171. doi:10.1080/13682820010019874. PMID 11344592.
- Sanjeevan, Teenu; Rosenbaum, David A.; Miller, Carol; van Hell, Janet G.; Weiss, Daniel J.; Mainela-Arnold, Elina (24 June 2015). "Motor Issues in Specific Language Impairment: a Window into the Underlying Impairment". Current Developmental Disorders Reports. 2 (3): 228–236. doi:10.1007/s40474-015-0051-9.
- Krishnan, Saloni; Watkins, Kate E.; Bishop, Dorothy V.M. (September 2016). "Neurobiological Basis of Language Learning Difficulties". Trends in Cognitive Sciences. 20 (9): 701–714. doi:10.1016/j.tics.2016.06.012. PMC 4993149. PMID 27422443.
- Herbert, Martha R.; Kenet, Tal (June 2007). "Brain Abnormalities in Language Disorders and in Autism". Pediatric Clinics of North America. 54 (3): 563–583. doi:10.1016/j.pcl.2007.02.007. PMID 17543910.
- Tomblin, J. Bruce; Records, Nancy L.; Zhang, Xuyang (December 1996). "A System for the Diagnosis of Specific Language Impairment in Kindergarten Children". Journal of Speech, Language, and Hearing Research. 39 (6): 1284–1294. doi:10.1044/jshr.3906.1284. PMID 8959613.
- Bishop, Dorothy V. M. (November 2017). "Why is it so hard to reach agreement on terminology? The case of developmental language disorder (DLD)". International Journal of Language & Communication Disorders. 52 (6): 671–680. doi:10.1111/1460-6984.12335. PMC 5697617. PMID 28714100.
- Identifying Red Flags for Developmental Language Disorder. (n.d.). Retrieved from https://www.boystownhospital.org/knowledge-center/red-flags-developmental-language-disorder.
- Paul, R. (2006). Language Disorders from Infancy through Adolescence: Assessment and Intervention, 3rd Edition. St. Louis: Mosby-Year Book.
- Roth, F. P., & Worthington, C. K. (2010). Treatment resource manual for speech-language pathology, 4th edition. San Diego: Singular Publishing.
- Ebbels, Susan (25 July 2016). "Teaching grammar to school-aged children with specific language impairment using Shape Coding". Child Language Teaching and Therapy. 23 (1): 67–93. doi:10.1191/0265659007072143. S2CID 49573186.
- Bryan, A., Colourful Semantics., in Language disorders in children and adults: psycholinguistic approaches to therapy., S. Chiat, J. Law, and J. Marshall, Editors. 1997, Whurr: London
- Gallagher, Tanya M. (1996). "Social-interactional approaches to child language intervention". In Beitchman, Joseph H.; Cohen, Nancy J.; Konstantareas, M. Mary; Tannock, Rosemary (eds.). Language, Learning, and Behavior Disorders: Developmental, Biological, and Clinical Perspectives. Cambridge University Press. pp. 418–435. ISBN 978-0-521-47229-6.
- Roberts, Megan Y.; Kaiser, Ann P. (1 August 2011). "The Effectiveness of Parent-Implemented Language Interventions: A Meta-Analysis". American Journal of Speech-Language Pathology. 20 (3): 180–199. doi:10.1044/1058-0360(2011/10-0055). PMID 21478280.
- Tosh, Rachel; Arnott, Wendy; Scarinci, Nerina (May 2017). "Parent-implemented home therapy programmes for speech and language: a systematic review". International Journal of Language & Communication Disorders. 52 (3): 253–269. doi:10.1111/1460-6984.12280. PMID 27943521.
- Archibald, Lisa MD (January 2017). "SLP-educator classroom collaboration: A review to inform reason-based practice". Autism & Developmental Language Impairments. 2: 239694151668036. doi:10.1177/2396941516680369.
- McCartney, Elspeth; Boyle, James; Ellis, Sue; Bannatyne, Susan; Turnbull, Mary (26 March 2010). "Indirect language therapy for children with persistent language impairment in mainstream primary schools: outcomes from a cohort intervention" (PDF). International Journal of Language & Communication Disorders. 46 (1): 74–82. doi:10.3109/13682820903560302. PMID 20337570.
- McCartney, Elspeth; Boyle, James; Ellis, Sue; Bannatyne, Susan; Turnbull, Mary (26 March 2010). "Indirect language therapy for children with persistent language impairment in mainstream primary schools: outcomes from a cohort intervention" (PDF). International Journal of Language & Communication Disorders. 46 (1): 74–82. doi:10.3109/13682820903560302. PMID 20337570.
- Law, James; Garrett, Zoe; Nye, Chad (August 2004). "The Efficacy of Treatment for Children With Developmental Speech and Language Delay/Disorder". Journal of Speech, Language, and Hearing Research. 47 (4): 924–943. doi:10.1044/1092-4388(2004/069). PMID 15324296.
- Boyle, James; McCartney, Elspeth; O'Hare, Anne; Law, James (November 2010). "Intervention for mixed receptive-expressive language impairment: a review" (PDF). Developmental Medicine & Child Neurology. 52 (11): 994–999. doi:10.1111/j.1469-8749.2010.03750.x. PMID 20813021. S2CID 34951225.
- Ebbels, Susan (9 December 2013). "Effectiveness of intervention for grammar in school-aged children with primary language impairments: A review of the evidence". Child Language Teaching and Therapy. 30 (1): 7–40. doi:10.1177/0265659013512321.
- Ebbels, Susan H.; Marić, Nataša; Murphy, Aoife; Turner, Gail (January 2014). "Improving comprehension in adolescents with severe receptive language impairments: a randomized control trial of intervention for coordinating conjunctions". International Journal of Language & Communication Disorders. 49 (1): 30–48. doi:10.1111/1460-6984.12047. PMID 24372884.
- Ebbels, Susan H.; Wright, Lisa; Brockbank, Sally; Godfrey, Caroline; Harris, Catherine; Leniston, Hannah; Neary, Kate; Nicoll, Hilary; Nicoll, Lucy; Scott, Jackie; Marić, Nataša (July 2017). "Effectiveness of 1:1 speech and language therapy for older children with (developmental) language disorder". International Journal of Language & Communication Disorders. 52 (4): 528–539. doi:10.1111/1460-6984.12297. PMID 27859986.
- Johnson, Carla J.; Beitchman, Joseph H.; Brownlie, E. B. (February 2010). "Twenty-Year Follow-Up of Children With and Without Speech-Language Impairments: Family, Educational, Occupational, and Quality of Life Outcomes". American Journal of Speech-Language Pathology. 19 (1): 51–65. doi:10.1044/1058-0360(2009/08-0083). PMID 19644128.
- Catts, Hugh W.; Fey, Marc E.; Tomblin, J. Bruce; Zhang, Xuyang (1 December 2002). "A Longitudinal Investigation of Reading Outcomes in Children With Language Impairments". Journal of Speech, Language, and Hearing Research. 45 (6): 1142–1157. doi:10.1044/1092-4388(2002/093). PMID 12546484.
- Snowling, Margaret J.; Adams, John W.; Bishop, D. V. M.; Stothard, Susan E. (2001). "Educational attainments of school leavers with a preschool history of speech-language impairments". International Journal of Language & Communication Disorders. 36 (2): 173–183. doi:10.1080/13682820120976. PMID 11344593.
- Simkin, Zoë; Conti-Ramsden, Gina (26 July 2016). "Evidence of reading difficulty in subgroups of children with specific language impairment". Child Language Teaching and Therapy. 22 (3): 315–331. doi:10.1191/0265659006ct310xx. S2CID 145300877.
- Botting, Nicola (March 2005). "Non-verbal cognitive development and language impairment". Journal of Child Psychology and Psychiatry. 46 (3): 317–326. doi:10.1111/j.1469-7610.2004.00355.x. PMID 15755307.
- Cohen, Nancy (2001). Language impairment and psychopathology in infants, children, and adolescents. Thousand Oaks: Sage Publications. ISBN 0-7619-2025-0. OCLC 45749780.
- Conti-Ramsden, Gina; Botting, Nicola (1 February 2004). "Social Difficulties and Victimization in Children With SLI at 11 Years of Age". Journal of Speech, Language, and Hearing Research. 47 (1): 145–161. doi:10.1044/1092-4388(2004/013). PMID 15072535.
- Clegg, J.; Hollis, C.; Mawhood, L.; Rutter, M. (February 2005). "Developmental language disorders - a follow-up in later adult life. Cognitive, language and psychosocial outcomes". Journal of Child Psychology and Psychiatry. 46 (2): 128–149. doi:10.1111/j.1469-7610.2004.00342.x. PMID 15679523.
- Snowling, Margaret J.; Bishop, D.V.M.; Stothard, Susan E.; Chipchase, Barry; Kaplan, Carole (9 June 2006). "Psychosocial outcomes at 15 years of children with a preschool history of speech-language impairment". Journal of Child Psychology and Psychiatry. 47 (8): 759–765. doi:10.1111/j.1469-7610.2006.01631.x. PMID 16898989.
- Tomblin, J. Bruce; Records, Nancy L.; Buckwalter, Paula; Zhang, Xuyang; Smith, Elaine; o'Brien, Marlea (1 December 1997). "Prevalence of Specific Language Impairment in Kindergarten Children". Journal of Speech, Language, and Hearing Research. 40 (6): 1245–1260. doi:10.1044/jslhr.4006.1245. PMC 5075245. PMID 9430746.
- Tomblin, J. Bruce; Records, Nancy L.; Buckwalter, Paula; Zhang, Xuyang; Smith, Elaine; O’Brien, Marlea (December 1997). "Prevalence of Specific Language Impairment in Kindergarten Children". Journal of Speech, Language, and Hearing Research. 40 (6): 1245–1260. doi:10.1044/jslhr.4006.1245. PMC 5075245. PMID 9430746.
- Bishop, D. V. M. (1997). Uncommon Understanding: Development and Disorders of Language Comprehension in Children. Hove: Psychology Press.
- Rice, Mabel L.; Wexler, Kenneth; Cleave, Patricia L. (1 August 1995). "Specific Language Impairment as a Period of Extended Optional Infinitive". Journal of Speech, Language, and Hearing Research. 38 (4): 850–863. doi:10.1044/jshr.3804.850. PMID 7474978.
- van der Lely, Heather K.J. (February 2005). "Domain-specific cognitive systems: insight from Grammatical-SLI". Trends in Cognitive Sciences. 9 (2): 53–59. doi:10.1016/j.tics.2004.12.002. PMID 15668097. S2CID 54374098.
- Gathercole, Susan E; Baddeley, Alan D (1 June 1990). "Phonological memory deficits in language disordered children: Is there a causal connection?". Journal of Memory and Language. 29 (3): 336–360. doi:10.1016/0749-596X(90)90004-J.
- Ullman, Michael T.; Pierpont, Elizabeth I. (1 January 2005). "Specific Language Impairment is not Specific to Language: the Procedural Deficit Hypothesis". Cortex. 41 (3): 399–433. doi:10.1016/S0010-9452(08)70276-4. PMID 15871604. S2CID 1027740.
- Bishop, Dorothy V. M. (2006). "Developmental cognitive genetics: How psychology can inform genetics and vice versa". Quarterly Journal of Experimental Psychology. 59 (7): 1153–1168. doi:10.1080/17470210500489372. PMC 2409179. PMID 16769616.
- Clegg, J.; Hollis, C.; Mawhood, L.; Rutter, M. (February 2005). "Developmental language disorders - a follow-up in later adult life. Cognitive, language and psychosocial outcomes". Journal of Child Psychology and Psychiatry. 46 (2): 128–149. doi:10.1111/j.1469-7610.2004.00342.x. PMID 15679523.
Further reading
External links
- Helpful article by Professor Maggie Snowling: Dyslexia and developmental language disorder: same or different?
- Raising Awareness of Language Learning Impairments (RALLI): Information about DLD via YouTube and Slideshare
- Talking Point: Check the progress of your child's language development
- What Works: Database of evidence-based interventions