Cryptococcus gattii
Cryptococcus gattii, formerly known as Cryptococcus neoformans var gattii, is an encapsulated yeast found primarily in tropical and subtropical climates. Its teleomorph is Filobasidiella bacillispora, a filamentous fungus belonging to the class Tremellomycetes.
| Cryptococcus gattii | |
|---|---|
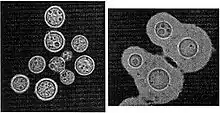 | |
| Cryptococcus neoformans weakly encapsulated (left) as it appears in nature, and (right) rehydrated with thick polysaccharide capsule as it appears once in the lungs. | |
| Scientific classification | |
| Kingdom: | |
| Phylum: | |
| Class: | |
| Order: | |
| Family: | |
| Genus: | |
| Species: | C. gattii |
| Binomial name | |
| Cryptococcus gattii (Vanbreus. & Takashio) Kwon-Chung & Boekhout | |
C. gattii causes the human diseases of pulmonary cryptococcosis (lung infection), basal meningitis, and cerebral cryptococcomas. Occasionally, the fungus is associated with skin, soft tissue, lymph node, bone, and joint infections. In recent years, it has appeared in British Columbia, Canada and the Pacific Northwest.[1] It has been suggested[2][3] that global warming may have been a factor in its emergence in British Columbia. It has also been suggested that tsunamis, such as the 1964 Alaska earthquake and tsunami, might have been responsible for carrying the fungus to North America and its subsequent spread there.[4] From 1999 through to early 2008, 216 people in British Columbia have been infected with C. gattii, and eight died from complications related to it.[5] The fungus also infects animals, such as dogs, koalas, and dolphins.[3] In 2007, the fungus appeared for the first time in the United States, in Whatcom County, Washington[6] and in April 2010 had spread to Oregon.[7] The most recently identified strain, designated VGIIc, is particularly virulent, having proved fatal in 19 of 218 known cases.[8]
Nomenclature
C. gattii has recently been divided into five species.[9] These are C. gattii, C. bacillisporus, C. deuterogattii, C. tetragattii, and C. decagattii.
Disease summary
Cryptococcal disease is a very rare disease that can affect the lungs (pneumonia) and nervous system (causing meningitis and focal brain lesions called cryptococcomas) in humans. The main complication of lung infection is respiratory failure. Central nervous system infection may lead to hydrocephalus, seizures, and focal neurological deficit.
Environmental occurrence
Soil debris associated with certain tree species has been found frequently to contain C. gattii VGIII MATα and MATa, and less commonly VGI MATα, in Southern California. These isolates were fertile, were found to be indistinguishable from the human isolates by genome sequence, and were virulent in in vitro and animal tests. Isolates were found associated with Canary Island pine (Pinus canariensis), American sweetgum (Liquidambar styraciflua), and Pohutukawa tree (Metrosideros excelsa).[10] Leading up to the study one of the authors, Scott Filler, sent his daughter Elan to obtain and culture fungal samples in the greater Los Angeles area; one of these turned out to be C. gattii.[11] Her work was presented at the Los Angeles County Science Fair, and she was credited as an author on the publication.[12]
Lead author Deborah Springer said, "Just as people who travel to South America are told to be careful about drinking the water, people who visit other areas like California, the Pacific Northwest, and Oregon need to be aware that they are at risk for developing a fungal infection, especially if their immune system is compromised."[13]
Epidemiology
The highest incidences of C. gattii infections occur in Papua New Guinea and Northern Australia. Cases have also been reported in other regions, indicating its spread to India, Brazil, Vancouver Island in Canada, and Washington, and Oregon in the United States.
Unlike Cryptococcus neoformans, C. gattii is not particularly associated with human immunodeficiency virus infection or other forms of immunosuppression. The fungus can cause disease in healthy people, potentially due to its ability to grow extremely rapidly within white blood cells.[14]
In the United States, C. gattii serotype B, subtype VGIIa, is largely responsible for clinical cases. The VGIIa subtype was responsible for the outbreaks in Canada; it then appeared in the U.S. Pacific Northwest.
According to a CDC summary, from 2004 to 2010, 60 cases were identified in the U.S.: 43 in Oregon, 15 from Washington, and one each from Idaho and California. Slightly more than half of these case were immunocompromised; 92% of all isolates were of the VGIIa subtype. In 2007, the first case in North Carolina was reported, subtype VGI, which is identical to the isolates found in Australia and California. In 2009, one case was identified in Arkansas.
The multiple clonal clusters in the Pacific Northwest likely arose independently of each other as a result of sexual reproduction occurring within the highly sexual VGII population.[15] VGII C. gattii have probably undergone either bisexual or unisexual reproduction in multiple different locales, thus giving rise to novel virulent phenotypes.
Transmission
The infection is caused by inhaling yeasts or spores. The fungus is not transmitted from person to person or from animal to person. A person with cryptococcal disease is not contagious.[16]
Symptoms
Most people who are exposed to the fungus do not become ill. In people who become ill, symptoms appear many weeks to months after exposure. Symptoms of cryptococcal disease include:
- Prolonged cough (lasting weeks or months)
- Sputum production
- Sharp chest pain
- Shortness of breath
- Sinusitis (cottony drainage, soreness, pressure)
- Severe headache (meningitis, encephalitis, meningoencephalitis)
- Stiff neck (prolonged and severe nuchal rigidity)
- Muscle soreness (mild to severe, local or diffuse)
- Photophobia (excessive sensitivity to light)
- Blurred or double vision
- Eye irritation (soreness, redness)
- Focal neurological deficit
- Fever (delirium, hallucinations)
- Confusion (abnormal behavior changes, inappropriate mood swings)
- Seizures
- Dizziness
- Night sweats
- Weight loss
- Nausea (with or without vomiting)
- Skin lesions (rashes, scaling, plaques, papules, nodules, blisters, subcutaneous tumors or ulcers)
- Lethargy
- Apathy
Diagnosis
Culture of sputum, bronchoalveolar lavage, lung biopsy, cerebrospinal fluid or brain biopsy specimens on selective agar allows differentiation between the five members of the C. gattii species complex and the two members of the C. neoformans species complex.
Molecular techniques may be used to speciate Cryptococcus from specimens that fail to culture.
Cryptococcal antigen testing from serum or cerebrospinal fluid is a useful preliminary test for cryptococcal infection, and has high sensitivity for disease. It does not distinguish between different species of Cryptococcus.
Treatment
Medical treatment consists of prolonged intravenous therapy (for 6–8 weeks or longer) with the antifungal drug amphotericin B, either in its conventional or lipid formulation. The addition of oral or intravenous flucytosine improves response rates. Oral fluconazole is then administered for six months or more.
Antifungals alone are often insufficient to cure C. gattii infections, and surgery to resect infected lung (lobectomy) or brain is often required. Ventricular shunts and Ommaya reservoirs are sometimes employed in the treatment of central nervous system infection.
People who have C. gattii infection need to take prescription antifungal medication for at least 6 months; usually the type of treatment depends on the severity of the infection and the parts of the body that are affected.
- For people who have asymptomatic infections or mild-to-moderate pulmonary infections, the treatment is usually fluconazole.
- For people who have severe lung infections, or infections in the central nervous system (brain and spinal cord), the treatment is amphotericin B in combination with flucytosine.[17]
See also
- Jenney A, Pandithage K, Fisher DA, Currie BJ (2004). "Cryptococcus infection in Tropical Australia". Journal of Clinical Microbiology. 42 (8): 3865–3868. CiteSeerX 10.1.1.627.3222. doi:10.1128/jcm.42.8.3865-3868.2004. PMC 497626. PMID 15297551.
References
- "Cryptococcus gattii Q&A". The Globe and Mail. 2007-02-10.
- Kidd, S.E.; F. Hagen; R. L. Tscharke; M. Huynh; K. H. Bartlett; M. Fyfe; L. MacDougall; T. Boekhout; K. J. Kwon-Chung; W. Meyer (December 7, 2004). "A rare genotype of Cryptococcus gattii caused the cryptococcosis outbreak on Vancouver Island (British Columbia, Canada)". Proceedings of the National Academy of Sciences of the United States of America. 101 (49): 17258–17263. Bibcode:2004PNAS..10117258K. doi:10.1073/pnas.0402981101. PMC 535360. PMID 15572442.
- Struck, Doug (2007-04-08). "Alien Invasion:The Fungus that came to Canada". The Washington Post.
- Johns Hopkins University, Bloomberg School of Health (October 1, 2019). "Did long ago tsunamis lead to mysterious, tropical fungal outbreak in Pacific northwest?". Phys.org. Science X Network. Retrieved October 3, 2019.
- "Deadly fungus migrates to Vancouver". Vancouver Sun. 2008-02-18. Archived from the original on 2012-11-04. Retrieved 2008-02-19.
- Rare, deadly tropical fungus moves into Whatcom County | KOMO-TV - Seattle, Washington | Local & Regional Archived 2007-10-17 at the Wayback Machine
- "Potentially deadly fungus spreading in U.S. and Canada". Reuters. 22 April 2010. Retrieved 2017-09-05.
- "New, Deadly Cryptococcus Gattii Fungus Found in U.S." 2010-04-23. Retrieved 2017-09-05.
- Hagen, Ferry; Khayhan, Kantarawee; Theelen, Bart; Kolecka, Anna; Polacheck, Itzhack; Sionov, Edward; Falk, Rama; Parnmen, Sittiporn; Lumbsch, H. Thorsten (2015-05-01). "Recognition of seven species in the Cryptococcus gattii/Cryptococcus neoformans species complex". Fungal Genetics and Biology. 78: 16–48. doi:10.1016/j.fgb.2015.02.009. ISSN 1096-0937. PMID 25721988.
- Deborah J. Springer; R. Blake Billmyre; Elan E. Filler; Kerstin Voelz; Rhiannon Pursall; Piotr A. Mieczkowski; Robert A. Larsen; Fred S. Dietrich; Robin C. May; Scott G. Filler; Joseph Heitman (August 21, 2014). "Cryptococcus gattii VGIII Isolates Causing Infections in HIV/AIDS Patients in Southern California: Identification of the Local Environmental Source as Arboreal". PLOS Pathogens. 10 (8): e1004285. doi:10.1371/journal.ppat.1004285. PMC 4140843. PMID 25144534.
- Karl Bates (2014-08-21). "Fungus deadly to AIDS patients found to grow on trees". Eurekalert.
- "California Trees Nailed As The Source Of Mystery Infections". WABE-TV. 2014-08-22. Archived from the original on 2014-08-26.
- "Fungus deadly to Aids patients grows on trees". Health24. 2014-08-22.
- Ma, H; Hagen, F; Stekel, DJ; Johnston, SA; Sionov, E; Falk, R; Polacheck, I; Boekhout, T; May, RC (4 August 2009). "The fatal fungal outbreak on Vancouver Island is characterized by enhanced intracellular parasitism driven by mitochondrial regulation". Proceedings of the National Academy of Sciences of the United States of America. 106 (31): 12980–5. Bibcode:2009PNAS..10612980M. doi:10.1073/pnas.0902963106. PMC 2722359. PMID 19651610.
- Billmyre RB, Croll D, Li W, Mieczkowski P, Carter DA, Cuomo CA, Kronstad JW, Heitman J. Highly recombinant VGII Cryptococcus gattii population develops clonal outbreak clusters through both sexual macroevolution and asexual microevolution. MBio. 2014 Jul 29;5(4):e01494-14. doi: 10.1128/mBio.01494-14. PMID 25073643
- Park, Alice (2010-04-23). "The 'Killer Fungus': Should We Be Scared?". Time. Retrieved 2010-04-23.
- "Clinical Practice Guidelines for Management of cryptococcal Disease: 2010 Update by Infectious Diseases Society of America" (PDF).
Further reading
- Buchanan, Kent; Murphy, Juneann W. (1998). "What Makes Cryptococcus neoformans a Pathogen?". Emerging Infectious Diseases. Centers for Disease Control and Prevention (CDC). 4 (1): 71–83. doi:10.3201/eid0401.980109. ISSN 1080-6040. PMC 2627665. PMID 9452400.
- Datta, Kausik; Bartlett, Karen H.; Baer, Rebecca; Byrnes, Edmond; Galanis, Eleni; Heitman, Joseph; Hoang, Linda; Leslie, Mira J.; MacDougall, Laura; Magill, Shelley S.; Morshed, Muhammad G.; Marr, Kieren A. (2009). "Spread of Cryptococcus gattii into Pacific Northwest Region of the United States". Emerging Infectious Diseases. Centers for Disease Control and Prevention (CDC). 15 (8): 1185–1191. doi:10.3201/eid1508.081384. ISSN 1080-6040. PMC 2815957. PMID 19757550.