African meningitis belt
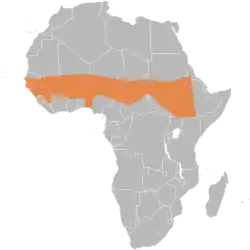
The African meningitis belt is a region in sub-Saharan Africa where the rate of incidence of meningitis is very high. It extends from Senegal to Ethiopia, and the primary cause of meningitis in the belt is Neisseria meningitidis.
The belt was first proposed by Léon Lapeyssonnie of the World Health Organization (WHO) in 1963. Lapeyssonnie noticed that the disease occurred in areas receiving 300-1,100 mm of mean annual rainfall, which is the case in sub-Saharan Africa.[1] The intercontinental spread of meningitis has also been traced to South Asia, brought by those making the haj, a pilgrimage to Saudi Arabia, in 1987, leading to epidemics in Nepal, Saudi Arabia, and Chad.[2]
Regions
It consists of part of or all of (from West to East), the Gambia, Senegal, Guinea-Bissau, Guinea, Mali, Burkina Faso, Ghana, Niger, Nigeria, Cameroon, Chad, Central African Republic, Sudan, South Sudan, Uganda, Kenya, Ethiopia, Eritrea. Many other countries in Africa experience outbreaks as well, but they are with less frequency and are less interepidemic. The "belt" has an estimated 300 million people in its total area. This region is not only prone to meningitis,[3] but also very prone to epidemics such as malaria.
The most affected countries in the region are Burkina Faso, Chad, Ethiopia, and Niger. Burkina Faso, Ethiopia, and Niger were accountable for 65% of all cases in Africa. In major epidemics, the attack rate range is 100 to 800 people per 100,000. However, communities can have attack rates as high as 1000 per 100,000. During these epidemics, young children have the highest attack rates.[4] More than 90,000 cases were reported in the belt in 2009, in comparison, less than 800 cases were reported in the United States[5] in 2011.
Epidemiology
Neisseria meningitidis is found in other parts of the world as well, but the highest rates occur in the “meningitis belt.” Meningococcal disease is persistently high in this region. Large epidemics occur every 5–12 years, typically during the dry season (December–June). Incidence of the disease declines from May to June in the more humid weather.[6] Other factors contributing to the sustained transmission of meningococcal disease include dust, other respiratory viruses that co-circulate, as well as close social contact.[7]
Historically, 90% of outbreaks in the meningitis belt were primarily due to Neisseria meningitidisserogroup A (NmA).[8] However, a monovalent serogroup A meningococcal conjugate vaccine (MenAfriVac) was introduced in the region in 2010. Since then, meningococcal outbreaks in the meningitis belt have primarily been due to serogroups C and W. A few serogroup X outbreaks have also been reported.[9]
In the African meningitis belt, the WHO defines a meningococcal epidemic as at least 100 cases per 100,000 inhabitants in a year.[10] At its peak, the incidence of meningococcal disease has reached rates of up to 1,000 cases per 100,000 inhabitants, such as during the epidemics of 1996 and 2000-2001.[11] In the belt, fatality from NmA disease has been estimated at 10-15%, although higher rates have been seen in some settings.[12] Around 10-20% of survivors of meningococcal meningitis are left with permanent neuropsychological conditions such as hearing loss, vision loss, epilepsy, or other neurological disorders. Young children are particularly vulnerable due to immaturity in their immune systems, which contributes to the disproportionate burden of the disease in Africa due to its young population.[13]
Meningitis vaccine
The Meningitis Vaccine Project was conceived in 2001 as an effort to stop the spread of meningitis in this region. As of June 2011, reports projected that the meningitis in this region would be under control with efficiency that local governments had desired.
References
- Lapeyssonnie, L. (November 1968). "[Comparative epidemiologic study of meningococcic cerebrospinal meningitis in temperate regions and in the meningitis belt in Africa. Attempt at synthesis]". Médecine Tropicale: Revue du Corps de Santé Colonial. 28 (6): 709–720. ISSN 0025-682X. PMID 5739513.
- Moore, P. S.; Reeves, M. W.; Schwartz, B.; Gellin, B. G.; Broome, C. V. (1989-07-29). "Intercontinental spread of an epidemic group A Neisseria meningitidis strain". Lancet. 2 (8657): 260–263. doi:10.1016/s0140-6736(89)90439-x. ISSN 0140-6736. PMID 2569063. S2CID 46601999.
- "Archived copy". Archived from the original on 2008-05-19. Retrieved 2009-10-20.CS1 maint: archived copy as title (link)
- "Archived copy". Archived from the original on 2014-04-29. Retrieved 2014-04-28.CS1 maint: archived copy as title (link)
- Murray, Patrick R.; Rosenthal, Ken S.; Pfaller, Michael A. (28 October 2015). Medical microbiology (8th ed.). Philadelphia, PA. ISBN 9780323299565. OCLC 914223501.
- Paireau, Juliette; Chen, Angelica; Broutin, Helene; Grenfell, Bryan; Basta, Nicole E (June 2016). "Seasonal dynamics of bacterial meningitis: a time-series analysis". The Lancet. Global Health. 4 (6): e370–e377. doi:10.1016/S2214-109X(16)30064-X. ISSN 2214-109X. PMC 5516123. PMID 27198841.
- Mustapha, Mustapha M.; Harrison, Lee H. (2018-01-16). "Vaccine prevention of meningococcal disease in Africa: Major advances, remaining challenges". Human Vaccines & Immunotherapeutics. 14 (5): 1107–1115. doi:10.1080/21645515.2017.1412020. ISSN 2164-5515. PMC 5989898. PMID 29211624.
- Lingani, Clément; Bergeron-Caron, Cassi; Stuart, James M.; Fernandez, Katya; Djingarey, Mamoudou H.; Ronveaux, Olivier; Schnitzler, Johannes C.; Perea, William A. (2015-11-15). "Meningococcal Meningitis Surveillance in the African Meningitis Belt, 2004-2013". Clinical Infectious Diseases. 61 Suppl 5: S410–415. doi:10.1093/cid/civ597. ISSN 1537-6591. PMC 4639499. PMID 26553668.
- "Meningococcal Disease - Chapter 4 - 2020 Yellow Book | Travelers' Health | CDC". wwwnc.cdc.gov. Retrieved 2020-11-18.
- World Health Organization. "Weekly epidemiological record" (PDF).
- Al-Tawfiq, Jaffar (2010). "Meningococcal Disease: The Organism, Clinical Presentation, and Worldwide Epidemiology". Journal of Travel Medicine. 7: 3–8. doi:10.1111/j.1708-8305.2010.00448.x. PMID 20849427.
- Greenwood, B. M.; Bradley, A. K.; Smith, A. W.; Wall, R. A. (1987). "Mortality from meningococcal disease during an epidemic in The Gambia, West Africa". Transactions of the Royal Society of Tropical Medicine and Hygiene. 81 (4): 536–538. doi:10.1016/0035-9203(87)90397-x. ISSN 0035-9203. PMID 3445333.
- Ramakrishnan, Meenakshi; Ulland, Aaron J; Steinhardt, Laura C; Moïsi, Jennifer C; Were, Fred; Levine, Orin S (2009-09-14). "Sequelae due to bacterial meningitis among African children: a systematic literature review". BMC Medicine. 7: 47. doi:10.1186/1741-7015-7-47. ISSN 1741-7015. PMC 2759956. PMID 19751516.
{kind=link}